



Forehead Lift (Brow Lift): Endotine vs. Bone Tunnel vs. Suture Fixation
Written by Yongwoo Lee MD, board-certified plastic surgeon specializing in facial rejuvenation surgeries at VIPPS
Forehead Lift Fixation Methods
When patients consult for a forehead lift or a brow lift in Korea, the conversation usually centers on incisions, recovery, and how natural the result will look. What they almost never hear about is the most consequential decision of the entire surgery: how the lifted forehead is going to be held in place.
This single technical choice determines how natural the result feels under the fingertips, whether a foreign object will sit beneath the scalp, and how comfortable the immediate recovery will be.
Three modern approaches exist: Endotine (a bioabsorbable polymer device), cortical bone tunnels (a suture threaded through holes drilled into the skull), and deep-tissue suture fixation (a suture anchored to the patient’s own scalp tissue, never touching bone). All three can produce a beautiful immediate lift. The differences emerge afterward.

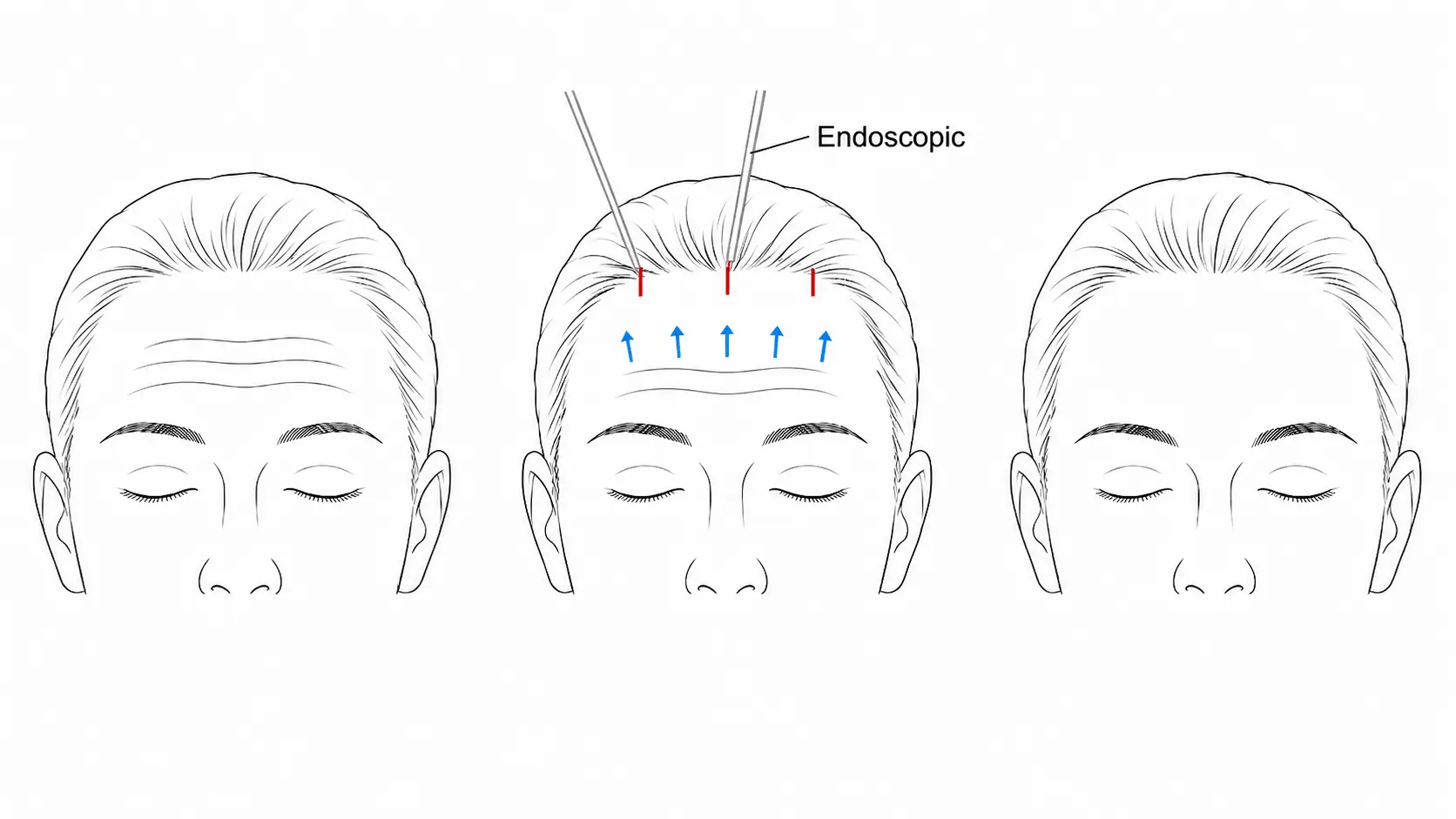
What an Endoscopic Forehead Lift Does
Through small incisions hidden in the hair-bearing scalp, an endoscope is used to release the forehead in the subperiosteal plane. Frown muscles can be selectively weakened. The forehead then slides upward into a more youthful position. The dissection itself is essentially the same regardless of fixation method. The fork in the road comes when the lifted tissue needs to be held in place while the body heals.
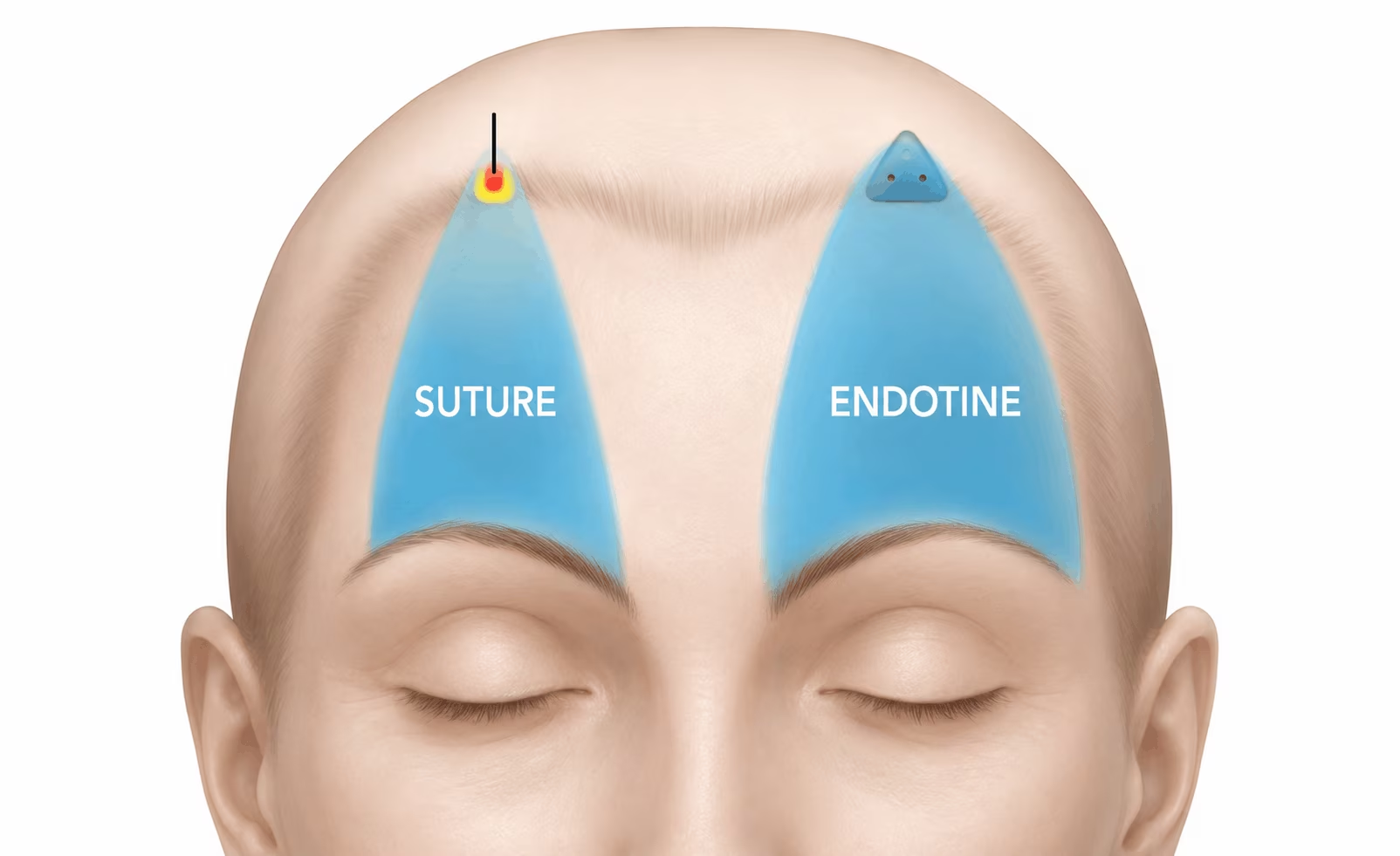
Method 1: Endotine Fixation
Endotine is a bioabsorbable polymer device with a post anchored in a shallow hole drilled in the skull, and five tines that grip the lifted scalp. Application takes about two minutes per side. But the same bulky device is the source of its problems:
- Palpability is the dominant complaint. In the original device study in Aesthetic Surgery Journal, Endotine was often palpable with moderate sensitivity. Later analyses found it was always palpable, and visible in roughly half of patients.
- It persists longer than expected, still palpable at 24 weeks after surgery in early studies. Newer polymers dissolve faster, but the foreign-body issue remains.
- Other documented issues: local inflammation, infection, extrusion through thin skin, device mobility, weaker lateral lift. The original Endotine was recalled by the FDA in 2003 due to drill bit safety concerns.
- It struggles with thick, heavy forehead tissue and adds material cost.
Endotine is not a bad device, but it solves the fixation problem by introducing a foreign object into the scalp, with all the trade-offs that follow.
Method 2: Cortical Bone Tunnel Fixation
The opposite approach: the surgeon drills two small holes into the outer cortex of the skull, angled to meet beneath a bridge of bone. A non-absorbable suture threaded through this tunnel is tied down to the lifted forehead. The literature, including Malata and Abood in the International Journal of Surgery, describes it as simple and reproducible. It removes the foreign body issue entirely. But drilling the skull introduces a different category of problems:
- Risk of intracranial penetration. In a study in American Journal of Otolaryngology, calvarial thickness ranged from 1.1 to 13.6 mm, thinnest precisely 1 cm anterior to the coronal suture, exactly where paramedian fixation is performed. Drilling depth must stay within 3 to 4 mm; violation carries a documented risk of cerebrospinal fluid (CSF) leak.
- Drilling vibration causes postoperative discomfort. Patients often report immediate headache, dizziness, and nausea (sometimes vomiting) from the percussive vibration through the calvarium.
- Technical complications: bone bridge fractures, brisk bleeding from the diploic space, occasional need to abandon a tunnel mid-procedure.
- Site-specific dysesthesia. Malata and Abood documented patients requiring suture removal six weeks postoperatively due to persistent nerve sensitivity at the bone fixation point.
- A small permanent osseous defect remains in the calvarium, visible on subsequent CT imaging.
Cortical bone tunnel fixation is legitimate and time-tested, but drilling into the skull is not a trivial intervention. The question becomes: can we gain the advantages of suture fixation without drilling the skull at all?
Method 3: Deep-Tissue Suture Fixation
The third approach anchors the suture into a band of the patient’s own deep, undisturbed scalp tissue posterior to the incision. The skull is never drilled. No foreign device is introduced.
A small main incision is made, identical to the other methods, with a second smaller puncture several centimeters posterior, where tissue remains firmly attached. A specialized instrument is passed through the posterior puncture into the main incision, where a heavy braided polyester suture is engaged and drawn back through the puncture. The instrument is then reintroduced through the same puncture a second time, intentionally piercing through a slip of deep, non-dissected tissue along its path, before returning to the incision to retrieve the other end. The suture’s middle loop is now anchored firmly through undisturbed deep tissue, and the two ends are tied down to the deep undersurface of the lifted forehead. The braided polyester suture remains permanently as a low-profile buried anchor while the body forms its own biological attachment. The scalp feels exactly like scalp.
Why Deep-Tissue Suture Has Become the Preferred Approach
A 2025 scoping review in Aesthetic Plastic Surgery emphasizes that the optimal endoscopic brow lift fixation combines durability, a clean patient experience, and minimal complications. Deep-tissue suture fixation meets each criterion at once:
- No foreign body in the scalp. The buried suture is biologically inert and impalpable.
- No drilling of the skull. No dural penetration risk, no CSF leak, no drill-related headache, no permanent osseous defect.
- Virtually impalpable. A 9-year experience study on related suture-based approaches reported no significant palpability issues.
- Durable and suitable for all anatomies, thick or thin foreheads.
The trade-off is honest: deep-tissue suture takes longer than Endotine and demands more surgical skill, but avoids the time and complexity of bone tunnel drilling, the slowest of the three.
Surgeon’s Insight
“When I examine a patient one year after surgery, I want them to feel nothing unusual when they touch their forehead. I want no memory of postoperative headache from drilling their skull. I want their result to belong entirely to their own anatomy. That is why deep-tissue suture fixation has become my default technique.“
Comparing the Three Fixation Methods Side by Side
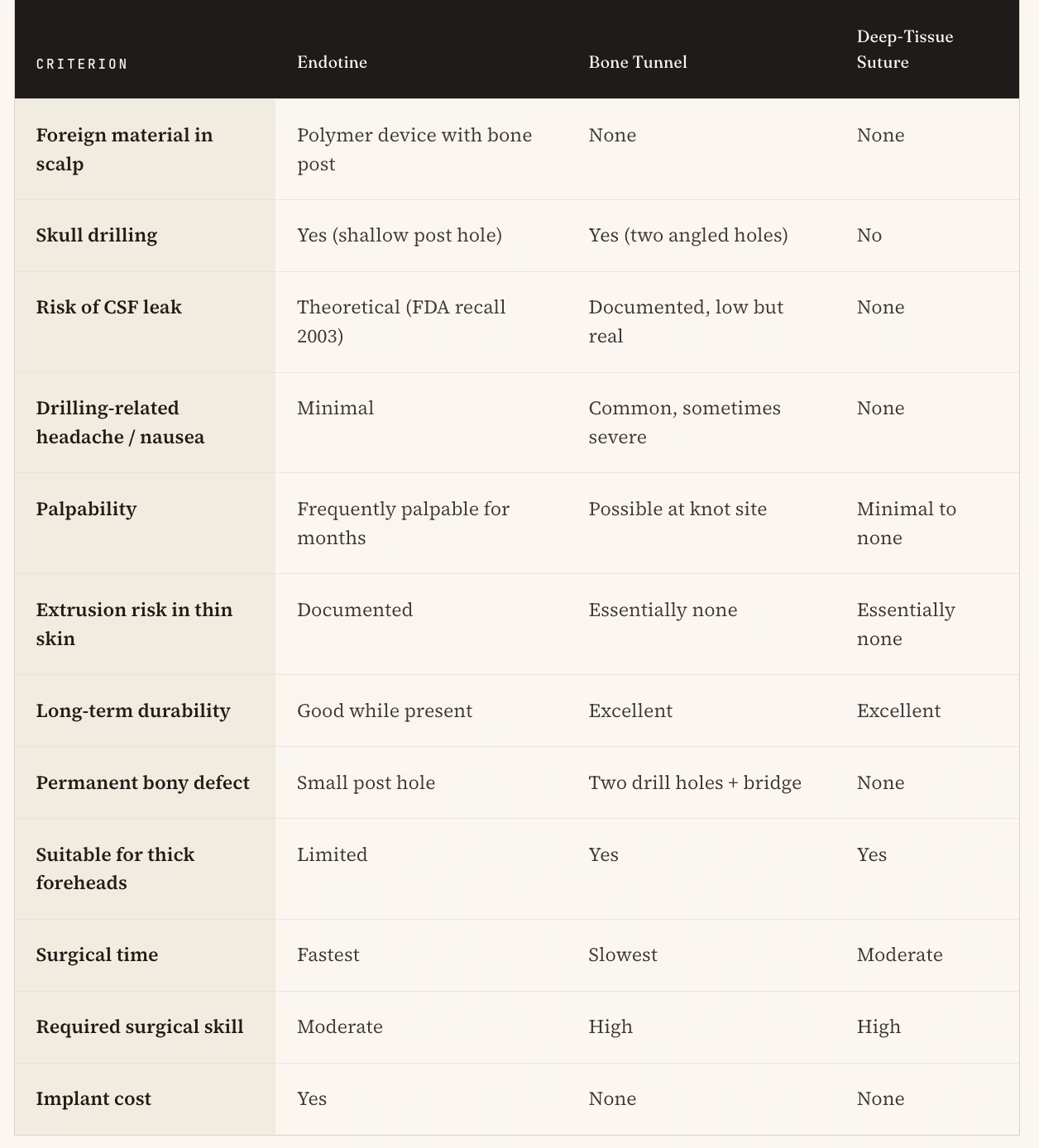
Endotine offers speed at the cost of a palpable foreign body. Bone tunnels offer rigid fixation at the cost of drilling the skull. Deep-tissue suture fixation offers the durability of suture-based anchoring without either trade-off.
Conclusion: The Best Fixation Is the One the Patient Never Notices
Both Endotine and cortical bone tunnel fixation solved real problems in their era. But the standard of what patients expect from modern aesthetic surgery has evolved. The result is now judged by how the patient experiences recovery, by whether anything feels different under the fingertips, and by what permanent alterations have been made to their anatomy.
Measured against that standard, deep-tissue suture fixation has become the most refined choice. Nothing to dissolve. Nothing to drill. No headache from skull vibration. No permanent hole in the cranium. A forehead held in place by the patient’s own anatomy, secured with a technique that demands more from the surgeon precisely so the patient is asked for less.
Frequently Asked Questions (FAQ)
Q1: Will I feel anything under my scalp after a suture-fixation forehead lift?
For the vast majority of patients, no. The only material is a buried surgical knot deep beneath thick scalp tissue. Most patients report normal sensation within a few weeks.
Q2: What is the safest fixation method for endoscopic forehead lift?
All three methods have established safety profiles in experienced hands. Deep-tissue suture fixation has the cleanest profile because it requires no skull drilling and no foreign device, eliminating risks of dural penetration, CSF leak, and implant complications.
Q3: Will drilling my skull cause headaches or nausea after the brow lift?
This is a specific concern with cortical bone tunnel fixation. Patients often describe immediate postoperative headache, dizziness, or nausea from the percussive vibration. With deep-tissue suture fixation, the skull is never touched and this category of symptoms does not occur.
Q4: Are the results of suture fixation permanent?
Yes. The suture holds the lifted tissue while the body forms biological attachments. The lift is then maintained by the patient’s own tissue, supported by the permanently buried suture.
Q5: What is the recovery time for an endoscopic forehead lift?
Most swelling resolves within seven to ten days. Patients typically return to work within fourteen days. Those who avoid bone drilling describe an easier first few days.
Q7: How do I choose the right surgeon for an endoscopic forehead lift in Korea?
Look for a board-certified plastic surgeon with demonstrated experience in endoscopic forehead lifting and modern fixation techniques. A surgeon who routinely performs related procedures such as upper blepharoplasty, deep plane facelift, and mini facelift likely has the broader anatomical experience that underpins refined brow lift technique in plastic surgery.
All procedures carry inherent risks. This content is for informational purposes only and does not constitute medical advice. Consult a board-certified plastic surgeon before making any medical decisions.







